In my efforts to help expedite your research on pediatric vaccines, here is one of the month 2 vaccines.
DTaP: Diphtheria, Tetanus, & acellular Pertussis
Diphtheria
Diphtheria is a bacterial infection caused by Corynebacterium diphtheriae. Once attached to the respiratory lining, the bacteria produces a toxin which kills healthy tissue. This creates a gray buildup of dead tissue that create a pseudomembrane within 2-3 days that can block the throat or other passageways making breathing and/or swallowing difficult. Toxin can also get into the bloodstream and cause problems with the heart, kidneys, and nerves. Other symptoms include: weakness, sore throat, fever, swollen glands. Severe cases lead to coma, paralysis, and death.
Diphtheria is spread via the air (cough/sneeze) or contact (toy/clothes/wound). It is typically spread in the winter and spring months. Without treatment, the person is contagious for 2-6 weeks. Risk factors for susceptibility to the disease are: overcrowding, poor health, substandard living conditions, incomplete immunization, and immunocompromised people. Infants are not typically susceptible to diphtheria as they care some immunity from in utero for 6-12 months, at which point this natural immunity wanes.
Tetanus
Tetanus is a bacterial infection caused by Clostridium tetani. The bacteria enters your body as a spore through a deep wound, incubation is 3-21 days (average of 10 days). The wound can be a puncture wound, burn, etc. This bacteria produces a toxin that bonds to your nerve endings and causes body wide muscle spasming. The toxin cannot be removed from your nerve endings and you need to grow new ones which can take several months. Complications of this disease are broken bones, pulmonary embolism, respiratory failure, and death.
Tetanus is found in soil, dust, and manure and is not spread from person to person. Although the bacteria is found world-wide, it is most prevalent in densely populated regions in hot, damp climates with soils rich in organic matter.
Pertussis
Pertussis is a highly contagious bacterial infection caused by Bordetella pertussis. The bacteria enters your body from contact with another person or respiratory droplets. An infected person is contagious for about 2 weeks after the cough begins. Even vaccinated people may be infected. Incubation is 5 days to 3 weeks. This bacteria produce a toxin that damages the cilia and cause airway swelling.
This disease looks very similar to a cold. In babies, the disease can cause apnea, or a pause in their breathing. This disease can be serious in babies and 50% of those that catch it will need to be hospitalized. After two weeks of infection that looks like a cold, the next 1-10 weeks are filled with terrible coughs that may be worse at night, make you have a ‘whooping’ inhale due empty lungs, vomiting and exhaustion are common after coughing fits. After this stage, there is a 2-4 week ‘recovery’ stage where there is less severe coughing and the symptoms are cold-like again; during this final stage people may be more susceptible to other respiratory infections. Primary natural immunity gained through infection lasts 4-20 years.
Statistics
Diphtheria
Before treatment and prevention methods were available, 50% of those infected died. In 1921, there were 206,000 cases and 15,520 deaths. Currently the case-fatality rate is 5-10%, up to 20% in those under 5 and over 40. Between 2004-2015 there were thankfully only 2 cases in the US. Worldwide, there were 4,778 cases in 2015. Since 1980, there has been no greater than 5 cases in the US annually. In recent times there have been outbreaks of the disease in eastern Europe and Russia.
Vaccination began in the 1920s in the US.
Tetanus
29 US reported cases 1996-2009. Tetanus is more of a problem in undeveloped areas of the world.
Vaccination began in the 1940s in the US.
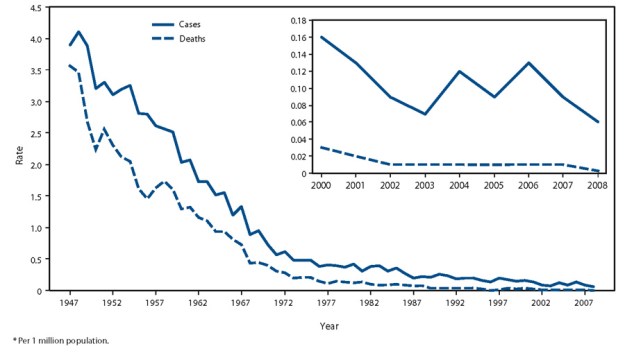
US Tetanus cases and deaths from 1900.
US Tetanus cases and deaths from 1947 per million people.
Pertussis
According to WHO, pertussis is a world-wide problem for infants, especially those in developing countries. Worldwide, they estimated 16 million cases in 2008, 95% were in developing countries. In 2008, 195,000 children died from pertussis. In 2008, 82% of world infants had 3 vaccinations for pertussis; the WHO goal is 90%. WHO states that “Although vaccination can prevent pertussis in adolescents and adults, there is insufficient evidence to support the addition of vaccine boosters in these age groups for achieving the primary goal of reducing severe pertussis in infants.”
Pertussis incidence was on a steady decline from the time reporting was mandatory in 1922. In recent times there has been an increase of pertussis in the US. Globally, there has also been a modern increase in incidence. The following figure illustrates this as well as when various versions of the vaccine were introduced. In 2014, there were 32,971 cases reported in the US.
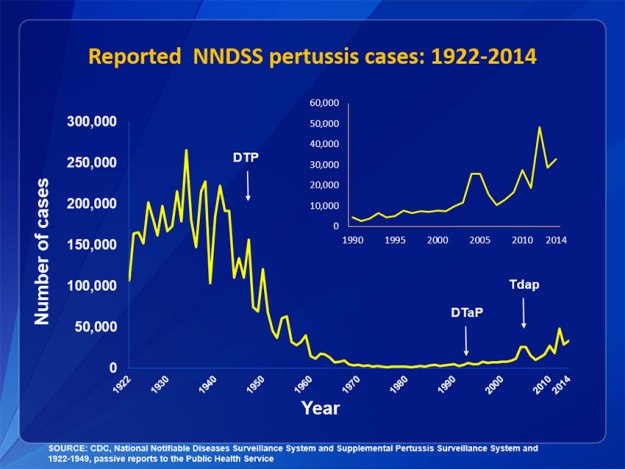
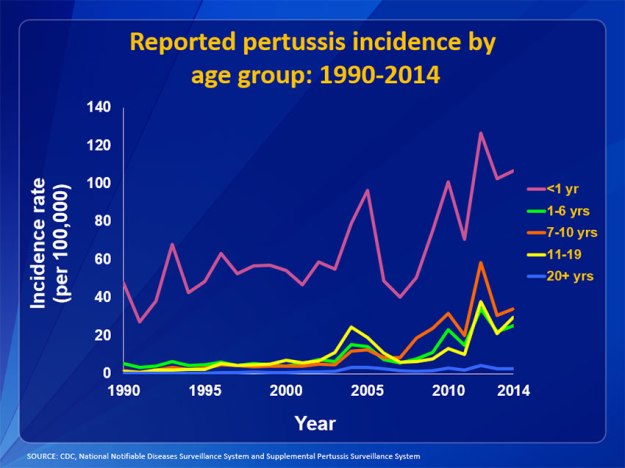
The following graph illustrates the modern increase by age group in the US.
How do you treat this disease?
Diphtheria
Even with treatment, diphtheria currently kills 3% of those that contract it. This rate is higher in those under age 15. Treatment typically involves ICU care and involves antitoxin and antibiotic treatments as well as possible removal of pseudomembrane blockages to the airways.
Tetanus
There is no cure for this disease. It is managed by injecting an anti-toxin which can block un-bonded toxin from binding to nerves. Antitoxins were discovered in the late 1800s and used in World War I. Antibiotics will be given to kill the bacteria. Sedatives and other drugs are given to decrease the spasming. Lengthy ICU stays are common and necessary to provide supportive care.
In 1984 there was a study in Bangladesh that utilized 1 gram of IV ascorbic acid (Vitamin C) in tetanus treatment, which was effective. There have been no follow-up studies on this.
Prevention is possible by thorough cleaning of wounds and leaving deep wounds open to the air. Tetanus thrives in an anaerobic environment. Neonatal tetanus is possible if birth occurs in a dirty environment. Neonatal tetanus is typically fatal.
Pertussis
Pertussis can be treated with antibiotics, but if you have been infected for over 3 weeks, they will not be helpful as a normal immune system will have already eliminated the bacteria from your body. Aside from following prescribed antibiotic directions, there are several things you can do to aid recovery: avoid airborne irritants such as smoke, chemical fumes, and dust, use a cool mist vaporizer, hydration, and good sanitary practices.
If a child is hospitalized, they may be given antibiotics and/or IV fluids. Keeping the airways clear and the child well-oxygenated is the key goal of hospital treatment.
How effective is this vaccine?
Since vaccination began in the 1920’s, diphtheria has significantly lessened the impact of the disease in the US and worldwide. A case-control study (conducted in 1993) in Russia during an outbreak demonstrated that 3 or more doses of the vaccine were 97% (94.3%-98.4%) effective. This same study showed 5-6 doses to be 99.0% (97.7%-99.6%) effective compared to unvaccinated children.
To date, there have been no studies done on the effectiveness of the tetanus vaccination.
The effectiveness of the pertussis vaccine is short-lived in most. A recent Canadian study on the acellular vaccine shows that those that are up-to-date with the pertussis vaccination have an 80% (71-86%) effectiveness within one year. From 1-3 years post vaccination (when up-to-date) the vaccine is 84% (77-89%) effective. After that, effectiveness drops dramatically as time passes. In those that are partially vaccinated, effectiveness is even lower.
Contraindications, Complications & Side-effects of DTaP vaccine
The CDC recommends postponing vaccination if your child is ill until after they recover from a current infection.
Children who have had a serious side effect or allergic reaction to a previous DTaP should not have another dose.
Any child who suffered a brain or nervous system disease within a week of prior vaccination should not be given further DTaP.
Special consideration should be taken before booster shots if with a previous DTaP injection, the child had a seizure, collapsed, cried non-stop for 3 hours, or had a fever over 105 degrees. For those children, having a version without pertussis may be better.
Side effects of the DTaP vaccine include: fever (25% of kids), redness/swelling in injection site (25% of kids), soreness at injection site (25% of kids). Swelling of entire extremity happens in later doses in 14% of kids. Other problems: fussiness (33% of kids) fatigue/anorexia (10% of kids), vomiting 2% of kids. All of these problems are common and occur within 1-3 days of the shot.
Other, more uncommon though more serious problems: seizures, 3 hours or more of constant crying, fever over 105 degrees, serious allergic reaction. Rare, severe long-term problems that have been reported include long-term seizures, lowered consciousness, coma, and permanent brain damage.
You are encouraged to go to the FDA site and read the inserts for the DTaP vaccine your child will be receiving.
Vaccine Injury Data: October 3, 2016
Data for DTaP only, not other versions or combination vaccines. Please go to http://www.hrsa.gov/vaccinecompensation/data/index.html for current data on various vaccines.
Claims filed: 494
Deaths: 80
Compensation Awarded: 205
Of note: to date, 39% of all compensated claims for vaccine injury were for versions of diphtheria, tetanus, and pertussis vaccines, including combination vaccines.
Adverse Reaction and reporting interval for VAERS:
- Anaphylaxis or anaphylactic shock (7 days)
- Brachial neuritis (28 days)
- Encephalopathy or encephalitis (7 days)
- Any acute complications or sequelae (including death) of above events (interval – not applicable)
- Events described in manufacturer’s package insert as contraindications to additional doses of vaccine (interval – see package insert)
Different versions of this vaccine
There are 6 branded versions of this vaccine and one generic. I will list the two that are actually DTaP here, the others add in other vaccines. The generic does not protect against pertussis.
Daptacel from Sanofi Pasteur. This version contains less aluminum and formaldehyde than the Infanrix.
Infanrix from GlaxoSmithKline.
I highly recommend you read the inserts of these on the CDC’s website when choosing the appropriate version for your child: http://www.cdc.gov/vaccinesafety/vaccines/dtap-tdap-vaccine.html
Timing of vaccination
The US recommended schedule is 5 doses at: 2 months, 4 months, 6 months, 15-18 months, and 4-6 years.
The Canadian recommended timeline varies among provinces, and includes 6 doses. They also use several different combo vaccines at different times. Children in Canada are recommended to have their doses at 2, 4, & 6 months, 18 months, age 4-6, and in 7-11th grade.
Alternative schedules:
2,4,& 6 months, 18 months, 4-6 years for DTap and then Tdap at age 10 with boosters every 5-10 years.
OR
2, 4, & 6 months, a Tetanus booster at age 7, and another Tetanus booster at age 17.
References:
Bisgard, KM, et al. 2000. Diphtheria toxoid vaccine effectiveness: a case-control study in Russia. The journal of infectious diseases, 181: S184-S187.
CDC
Clark, TA. 2014. Changing pertussis epidemiology: everything old is new again. Journal of infectious diseases, 209: 978-981.
Jahan, K, et al. 1984. Effect of ascorbic acid in the treatment of tetanus. Bangladesh Medical Resource Council Bulletin, 10: 24-28.
Mayo Clinic
Medscape summary of Diphtheria, by Bruce Lo et. al.
Schwartz, K.L. 2016. Effectiveness of pertussis vaccination and duration of immunity. CMAJ, published online September 2016, early release.
WHO
Alternative schedule information from pediatrician websites.
